Biography
Biostatistician with more than 6 years of experience working in the field of clinical trials. Primary therapeutic areas of interest are CVRM (cardiovascular, renal and metabolism). Experience in contributing to the development of the statistical strategy, overseeing the technical activities related to design, delivery and interpretation, as well as participating in high level internal governance committees and regulatory submissions of a project, and representing Biometrics in cross-functional collaborations. Teaching experience from Le Mans University, American University of Armenia and Yerevan State University. The main taught courses are Statistics and Data Science with R. Research interests are in the field of Statistics of Stochastic Processes.
Interests
- Statistics
- Data Science with R
- Clinical Trials
Education
-
PhD in Mathematical Statistics, 2016
Le Mans University, France
-
MSc in Theory of Probability and Mathematical Statistics, 2012
Yerevan State University, Armenia
-
BSc in Mathematics, 2010
Yerevan State University, Armenia
Experience
Statistician
AstraZeneca
Statistician working in Phase 3 cardiovascular outcome trials:
- Writing the statistical sections of the protocol
- Creating the Statistical Analysis Plan (SAP)
- Overall design and implementation of analysis and reporting
Lecturer
Yerevan State University
Biostatistician
FMD K&L Inc. (ClinChoice Inc.)
Responsibilities include:
- Assisting in the implementation of protocol methodology and Statistical Analysis Plans (SAP)
- Contributing to decision making on design and data collection ensuring alignment with trial objectives
- Validating TLG (Tables, Listings, Graphs) programming, ADaM datasets and mapping specifications
ATER (Attaché Temporaire d’Enseignement et de Recherche)
Le Mans Université
Recent Posts
Maraca Plots - Basic Usage
Neyman-Pearson and some other Uniformly Most Powerful Tests
Bayesian Estimation
Win Odds Confidence Intervals in R
Projects
Armdown
Producing Scientific Documents in Armenian.

EasySTAT Project
EasyStat App is an R based FREE web application. This platform can help you to independently conduct research data analyses.
Recent & Upcoming Talks
Design and analysis of studies based on hierarchical composite endpoints: Insights from the DARE-19 trial





Featured Publications
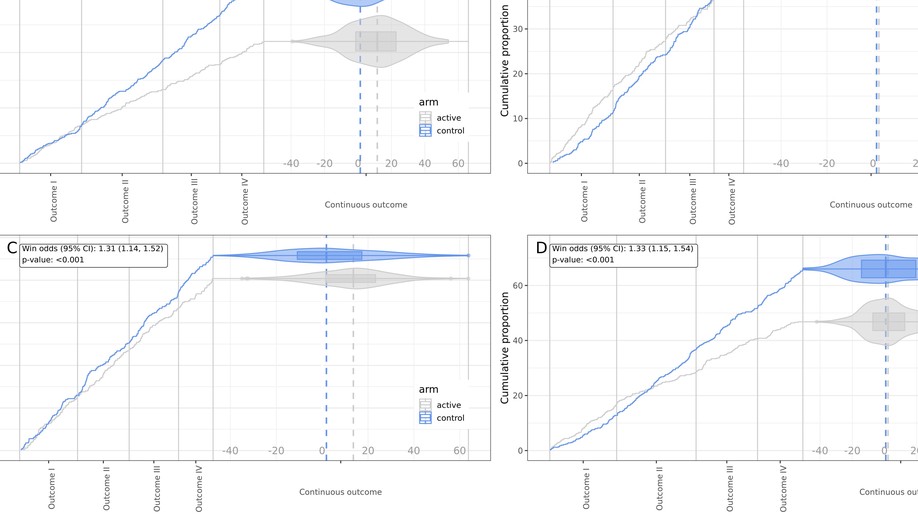
The maraca plot: A novel visualization of hierarchical composite endpoints
Background: Hierarchical composite endpoints are complex endpoints combining outcomes of different types and different clinical importance into an ordinal outcome that prioritizes the clinically most important (e.g. most severe) event of a patient. Hierarchical composite endpoint can be analysed with the win odds, an adaptation of win ratio to include ties. One of the difficulties in interpreting hierarchical composite endpoint is the lack of proper tools for visualizing the treatment effect captured by hierarchical composite endpoint, given the complex nature of the endpoint which combines events of different types. Methods: Hierarchical composite endpoints usually combine time-to-event outcomes and continuous outcomes into a composite; hence, it is important to capture not only the shift from more severe categories to less severe categories in the active group in comparison to the control group (as in any ordinal endpoint), but also changes occurring within each category. We introduce the novel maraca plot which combines violin plots (with nested box plots) to visualize the density of the distribution of the continuous outcome and Kaplan–Meier plots for time-to-event outcomes into a comprehensive visualization. Conclusion: The novel maraca plot is suggested for visualization of hierarchical composite endpoints consisting of several time-to-event outcomes and a continuous outcome. It has a very simple structure and therefore easily communicates both the overall treatment effect and the effect on individual components.
- The maraca plot: A novel visualization of hierarchical composite endpoints was published in Clinical Trials.
Dapagliflozin across the range of ejection fraction in patients with heart failure: a patient-level, pooled meta-analysis of DAPA-HF and DELIVER
Whether the sodium–glucose cotransporter 2 inhibitor dapagliflozin reduces the risk of a range of morbidity and mortality outcomes in patients with heart failure regardless of ejection fraction is unknown. A patient-level pooled meta-analysis of two trials testing dapagliflozin in participants with heart failure and different ranges of left ventricular ejection fraction (≤40% and >40%) was pre-specified to examine the effect of treatment on endpoints that neither trial, individually, was powered for and to test the consistency of the effect of dapagliflozin across the range of ejection fractions. The pre-specified endpoints were: death from cardiovascular causes; death from any cause; total hospital admissions for heart failure; and the composite of death from cardiovascular causes, myocardial infarction or stroke (major adverse cardiovascular events (MACEs)). A total of 11,007 participants with a mean ejection fraction of 44% (s.d. 14%) were included. Dapagliflozin reduced the risk of death from cardiovascular causes (hazard ratio (HR) 0.86, 95% confidence interval (CI) 0.76–0.97; P=0.01), death from any cause (HR 0.90, 95% CI 0.82–0.99; P=0.03), total hospital admissions for heart failure (rate ratio 0.71, 95% CI 0.65–0.78; P<0.001) and MACEs (HR 0.90, 95% CI 0.81–1.00; P=0.045). There was no evidence that the effect of dapagliflozin differed by ejection fraction. In a patient-level pooled meta-analysis covering the full range of ejection fractions in patients with heart failure, dapagliflozin reduced the risk of death from cardiovascular causes and hospital admissions for heart failure (PROSPERO: CRD42022346524).
- Dapagliflozin across the range of ejection fraction in patients with heart failure: a patient-level, pooled meta-analysis of DAPA-HF and DELIVER was published in Nature Medicine (2022): 28 (9), 1956–1964.
Power and sample size calculation for the win odds test: application to an ordinal endpoint in COVID-19 trials
The win odds is a distribution-free method of comparing locations of distributions of two independent random variables. Introduced as a method for analyzing hierarchical composite endpoints, it is well suited to be used in the analysis of ordinal scale endpoints in COVID-19 clinical trials. For a single outcome, we provide power and sample size calculation formulas for the win odds test. We also provide an implementation of the win odds analysis method for a single ordinal outcome in a commonly used statistical software to make the win odds analysis fully reproducible.

Dapagliflozin in patients with cardiometabolic risk factors hospitalised with COVID-19 (DARE-19)
DARE-19 was a randomised, double-blind, placebo-controlled trial of patients hospitalised with COVID-19 and with at least one cardiometabolic risk factor (ie, hypertension, type 2 diabetes, atherosclerotic cardiovascular disease, heart failure, and chronic kidney disease). Patients were randomly assigned 1:1 to dapagliflozin (10 mg daily orally) or matched placebo for 30 days.
Adjusted win ratio with stratification: Calculation methods and interpretation
The win ratio is a general method of comparing locations of distributions of two independent, ordinal random variables, and it can be estimated without distributional assumptions. In this paper we provide a unified theory of win ratio estimation in the presence of stratification and adjustment by a numeric variable.

Publications related to the PhD thesis
This work is devoted to the questions of the statistics of stochastic processes. Particularly, the first chapter is devoted to a non-parametric estimation problem for an inhomogeneous Poisson process. The second chapter is dedicated to a problem of estimation of the solution of a Backward Stochastic Differential Equation (BSDE).
Recent Publications
The maraca plot: A novel visualization of hierarchical composite endpoints
Background: Hierarchical composite endpoints are complex endpoints combining outcomes of different types and different clinical …

Dapagliflozin across the range of ejection fraction in patients with heart failure: a patient-level, pooled meta-analysis of DAPA-HF and DELIVER
Whether the sodium–glucose cotransporter 2 inhibitor dapagliflozin reduces the risk of a range of morbidity and mortality outcomes in …

Comments on 'Sample size formula for a win ratio endpoint' by RX Yu and J. Ganju
We compared two recently published formulas for the sample size calculation based on the win ratio and the win odds tests. Both are …

Design and Analysis of Studies Based on Hierarchical Composite Endpoints: Insights from the DARE-19 Trial

Dapagliflozin and Kidney Outcomes in Hospitalized Patients with COVID-19 Infection
